さまざまな種類の脳腫瘍に対して、脳への損傷を最小限に抑える鍵穴手術から頭蓋底部のアプローチ方法など様々な手法での手術を行っています。
また、手術での摘出リスクが高い部位に関しては定位放射線手術を併用することにより、より安全な治療戦略を提案します。
I perform neurosurgical procedures, which includes using key hole approach or extended skull base approach, based on the brain tumor size and location. For tumors located in high risk regions, Gamma Knife therapy may be done after the surgery to enhance safety and effectiveness.
小さな腫瘍の場合は、ガンマナイフ治療のみでも治療が可能です。中くらいのサイズを超える場合は、安全を優先に考えた手術を行います。通常は耳の後ろから、4~6cmの皮膚切開で500円玉程度の開頭部より摘出を行います。手術は腫瘍のサイズによりますが、3~5時間程度必要です。必要に応じて残存部にガンマナイフ治療を追加します。
For small tumors, Gamma Knife surgery is solely used for treatment. Moderate-sized tumors can be excised completely with maximum safety with neuromonitoring and post-operative Gamma Knife if necessary. In most cases, the surgery is performed through retroauricular region with small skin incision of ~4-6 cm and less than 3 cm craniotomy in diameter.
頭蓋内のあらゆる部位に発生する可能性のある腫瘍です。腫瘍の部位により、治療選択は異なります。手術で全摘出が理想的ですが、手術のリスクが高い部分はガンマナイフ治療を併用します。頭蓋底部にできた腫瘍の場合は、頭蓋底からの特殊なアプローチが必要なこともあります。
This type of tumor may develop in any region in the skull where the dura mater overlies the brain. The strategy differs according to the location and size. Due to the benign nature, total removal with the originating dura mater is ideal. However, some tumors arising from the skull base require skull base approach and post-operative Gamma Knife.
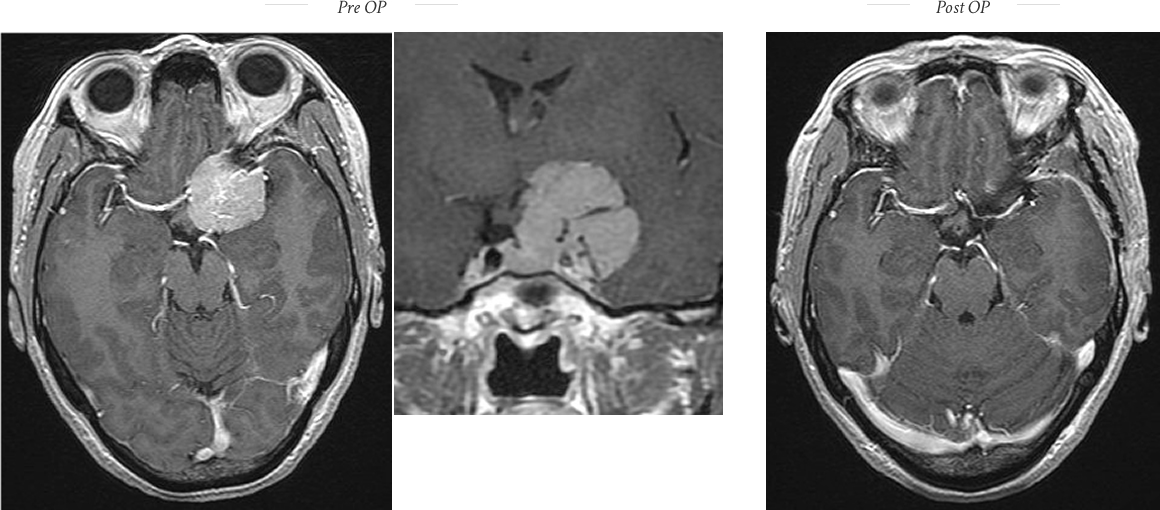
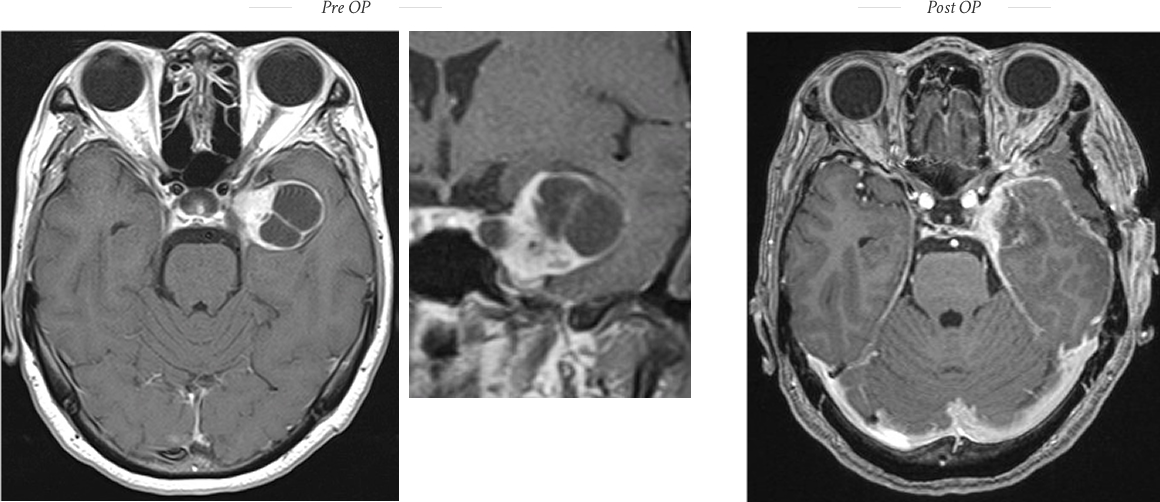
視神経付近にできることが多く、目の症状を生じることが多い腫瘍です。 手術で全摘出できれば治癒しますが、腫瘍の両側には内頸動脈、海綿静脈洞、脳神経が走行しており、綿密な治療計画と繊細な治療が必要です。耳鼻咽喉科・鼻内視鏡のエキスパートが鼻から頭蓋底部までのアプローチを行った後に、頭蓋骨底部に1円玉程度の小さい開頭を行い、腫瘍の摘出を行います。治療は3時間程度終了します。切開は鼻の奥で行いますので、手術創が外から見えることはありません。
These tumors commonly show symptoms of visual disturbance as they arise around the optic nerves. Total removal leads to complete cure, however, it requires multiple techniques such as microsurgical technique and endoscopic surgery. Small craniotomy less than 2 cm in diameter is made at the middle of the skull base. All procedures are completed within 2-3 hours. The skin incision made inside the nostril cannot be seen after the operation.
まれな腫瘍ですが、三叉神経痛を来すことがあり、ある程度の大きさの腫瘍の場合は摘出が必要です。鍵穴手術から特殊な開頭を必要とする場合など、患者さんに応じた治療方法を検討します。
This is a rare intracranial tumor. This tumor frequently causes trigeminal neuralgia as it tends to arise around the trigeminal nerve. The extent of removal is determined by the symptoms. Due to its benign nature, some patients only require partial removal around the trigeminal nerve for trigeminal neuralgia.
悪性腫瘍(肺癌、乳癌など)が脳に転移をきたすことがあります。 ガンマナイフ治療が極めて有効ですが、大きな場合は手術で摘出することもあります。
Malignant tumors (lung cancer, breast cancer) may metastasize to the brain. Gamma Knife is the most effective option to control this kind of tumor. For large tumors, initial surgical removal, followed by Gamma Knife is a reasonable treatment choice.
Dr. Takuro Inoue, trusted by patients from over 30 countries for microvascular decompression (MVD), now leads a certified Gamma Knife team delivering the same world-class precision and care.
Dr. Takuro Inoue is a board-certified neurosurgeon with over 30 years of experience. Known worldwide for his expertise in microvascular decompression (MVD), he has welcomed patients from more than 30 countries across North America, Europe, Asia, and the Middle East.
For more than two decades, Dr. Inoue and the Gamma Knife team at Koto Memorial Hospital collaborated with the late Dr. Takanori Fukushima, a legendary neurosurgeon renowned worldwide for his mastery of skull base surgery. Together, they developed a unique treatment approach combining advanced skull base surgery with Gamma Knife radiosurgery.
Patients at Koto Memorial Hospital receive Gamma Knife radiosurgery at a significantly lower cost than in many countries — only ¥800,000 (~USD 5,000) for international patients. This price includes the extra coordination and support required for overseas visitors, while remaining far below international rates.
Gamma Knife technology is produced by a single global manufacturer, Elekta, ensuring a high level of precision when the system is properly maintained. At Koto Memorial Hospital, we exceed global maintenance standards by performing accuracy checks and comprehensive servicing more than four times per year under a direct contract with Elekta.
What sets Koto apart is not only our technical excellence, but also our decades of experience in international patient care. Dr. Inoue’s career in microvascular decompression has brought patients from over 30 countries to Japan, giving our team unmatched experience in supporting people traveling for complex neurosurgical procedures.
We also maintain a close partnership with the National Brain Center Hospital (RSPON) in Jakarta, offer follow-up, and integrate skull base surgical expertise with radiosurgery — benefits rarely available at other centers.
Koto Memorial Hospital has a long-standing collaboration with the National Brain Center Hospital (RSPON) in Jakarta, Indonesia.
In partnership with Dr. Ryan Keswani, M.D., Dr. Sayyid Abdil Hakam Perkasa, M.D., and Dr. Abrar Arham, M.D., we have shared expertise in Gamma Knife radiosurgery and neurosurgical care for many years.
Through this cooperation, patients in Indonesia can receive pre-treatment consultations and evaluations at RSPON, ensuring a smooth referral process to our facility in Japan for advanced Gamma Knife treatment when needed. After treatment at Koto Memorial Hospital, patients can benefit from follow-up care at RSPON.
“I came to Japan for MVD with Dr. Inoue years ago. When I later needed Gamma Knife treatment, I returned without hesitation. The care from Dr. Inoue and his team was once again world-class.”
– Emily W., USA
We accept applications exclusively through the email link below.
53 F
Incidental case
Neurologically intact
Total removal without neurological deficit
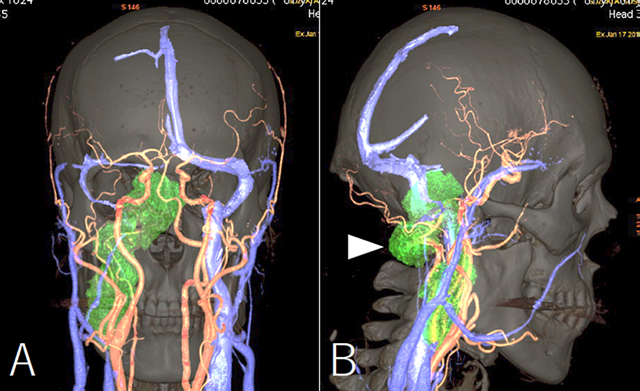
66 F
Visual disturbance
Pre Op Embolization
Subtotal removal
Post Op
Improved visual function
No oculomotor palsy
Remnant followed by GK
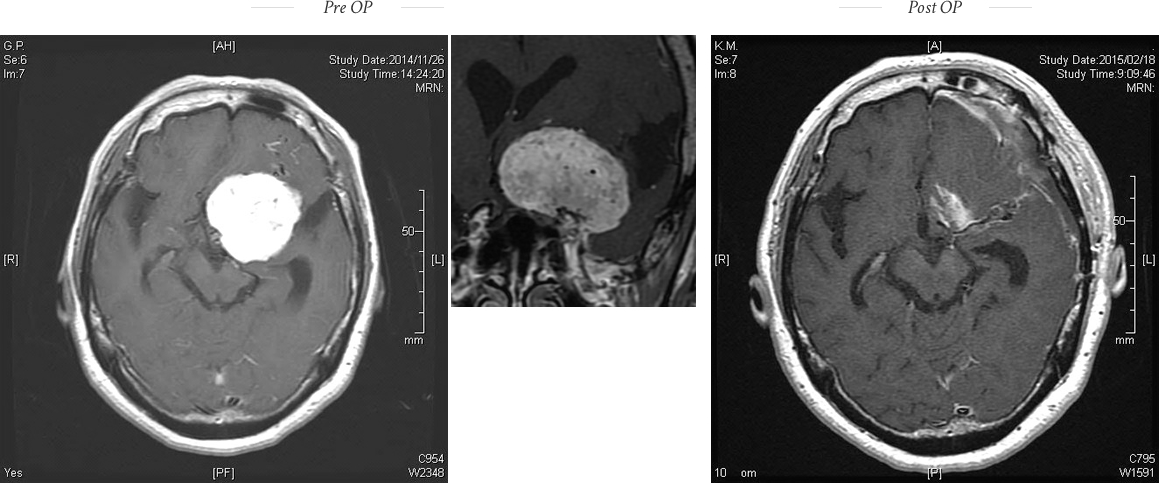
She was diagnosed with this meningioma 10 years ago, which gradually grew to large size. Increased intracranial pressure due to hydrocephalus impaired her vision. After internal decompression, she was treated with Gamma Knife thereafter.
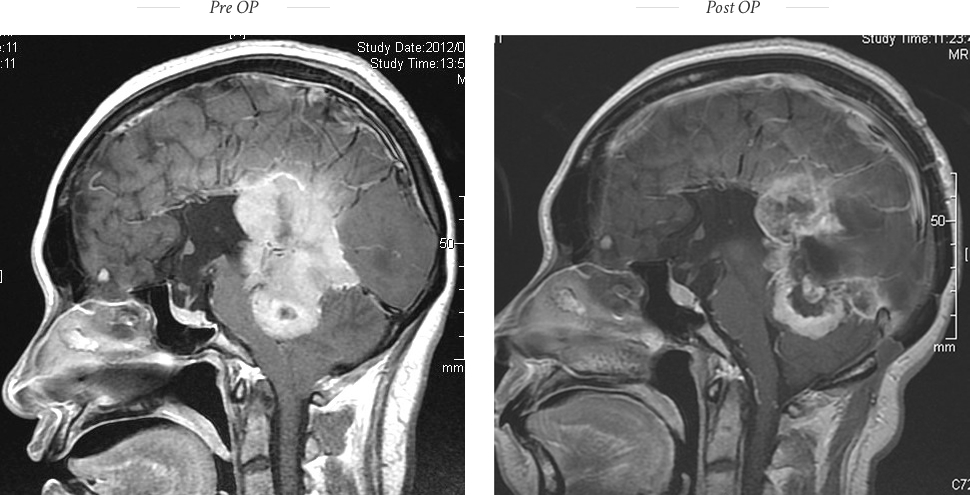
67 M
Motor weakness of the right side, gait disturbance and poor activity.
After removal, he regained his activity and disappearance of the weakness.
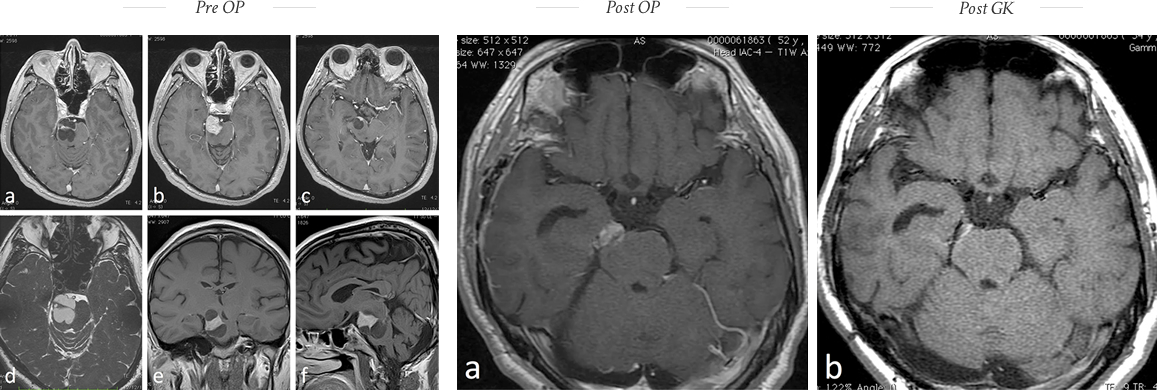
59 F
Incidental case, Neurologically intact
Temporopolar approach
No deficit
Cavernous remnant followed by GK
A 52-year-old man suffered from diplopia, gait disturbance, and sensory disturbance. MR imaging demonstrated a large cystic mass at ambient cistern on the right side.
Subtotal excision followed by Gamma Knife surgery was undertaken. His neurological symptoms disappeared with radiological reduction in size at 15 months follow-up.
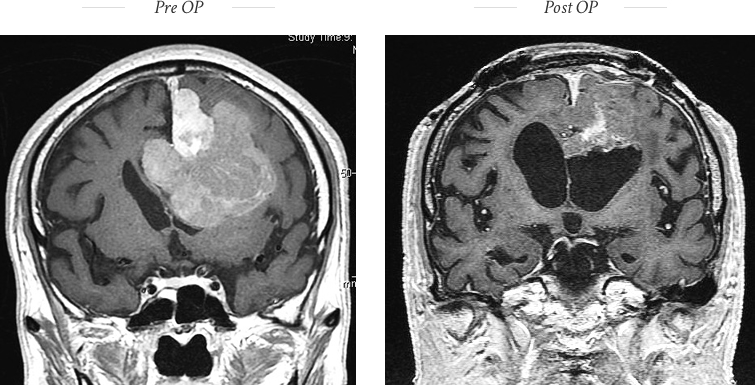
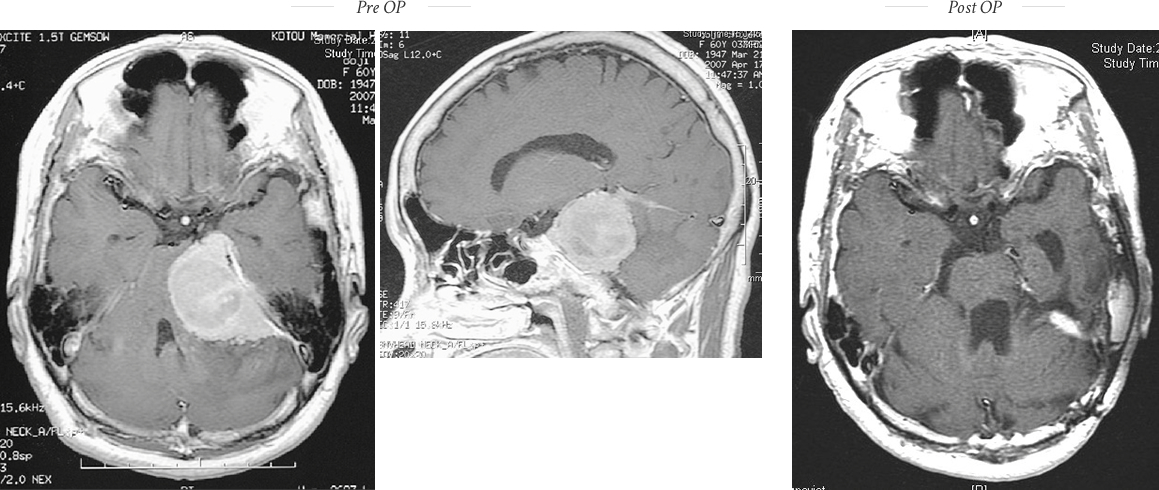
60 F
Progressive motor weakness of right side, gait disturbance, and hearing loss, eventually leading to complete bed rest.
After total removal, she was able to walk and lives a normal life except the deafness.
70 F
She was twice operated at other hospital.
However, the tumor regrew rapidly. Total removal of the tumor was performed with extended skull base technique, followed by facial nerve reconstruction using sural nerve graft.
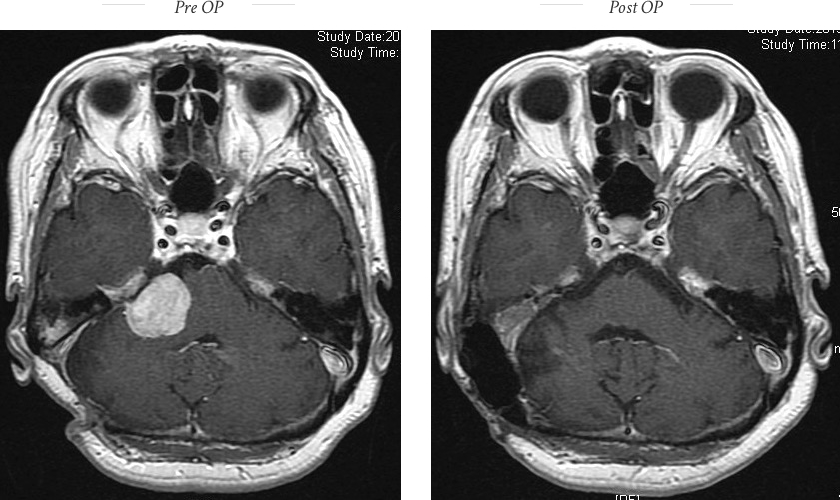
A 61-year-old male with a large hypoglossal schwannoma with moderate tongue atrophy.
The tumor extended from the enlarged hypoglossal canal to the brainstem intradurally and the high cervical region extradurally. Through the extreme lateral infrajugular transcondylar (ELITE) skull base approach, the tumor was completely removed in a single-stage operation.
※要予約※Reservation required.
| 湖東記念病院 Koto Memorial HospitalWebSite |
平日 Weekdays |
午後 p.m. |
| 学研都市病院 Gakkentoshi HospitalWebSite |
第3土曜日 Third Saturday |
午前 a.m. |
| 蘇生会総合病院 Soseikai HospitalWebSite |
第3土曜日 Third Saturday |
午後 p.m. |
| 湖東記念病院 Koto Memorial HospitalWebSite |
日本、滋賀 Shiga, Japan |
| 蘇生会総合病院 Soseikai General HospitalWebSite |
日本、京都 Kyoto, Japan |
| 志太記念脳神経外科 Shida Memorial Neurosurgery ClinicWebSite |
日本、静岡 Shizuoka, Japan |
| Andalusia HospitalWebSite | Alexandria, Egypt |
| National Brain Center HospitalWebSite | Jakarta, Indonesia |
湖東記念病院脳神経外科主任部長
日本脳神経外科学会専門医